Mass micronutrient deficiency is invisible. In talking to a dozen data collectors from seven nonprofits, we realized this invisibility makes it challenging for them to know where to establish fortification/supplementation interventions. As a result, they must collect thousands of blood samples and perform lab tests.
In Nigeria, it is estimated that 32% of the population has severe micronutrient deficiency, however 80% of them are not receiving treatment. Data on at-risk populations (women +children) is being collected on a 20-40 year basis, and consequently, micronutrient deficiency continues to remain invisible. The high costs of shipping blood samples overseas , and the lab tests ($15-60 USD per biomarker) themselves are the main barrier to collecting more actionable data (<$10M total).
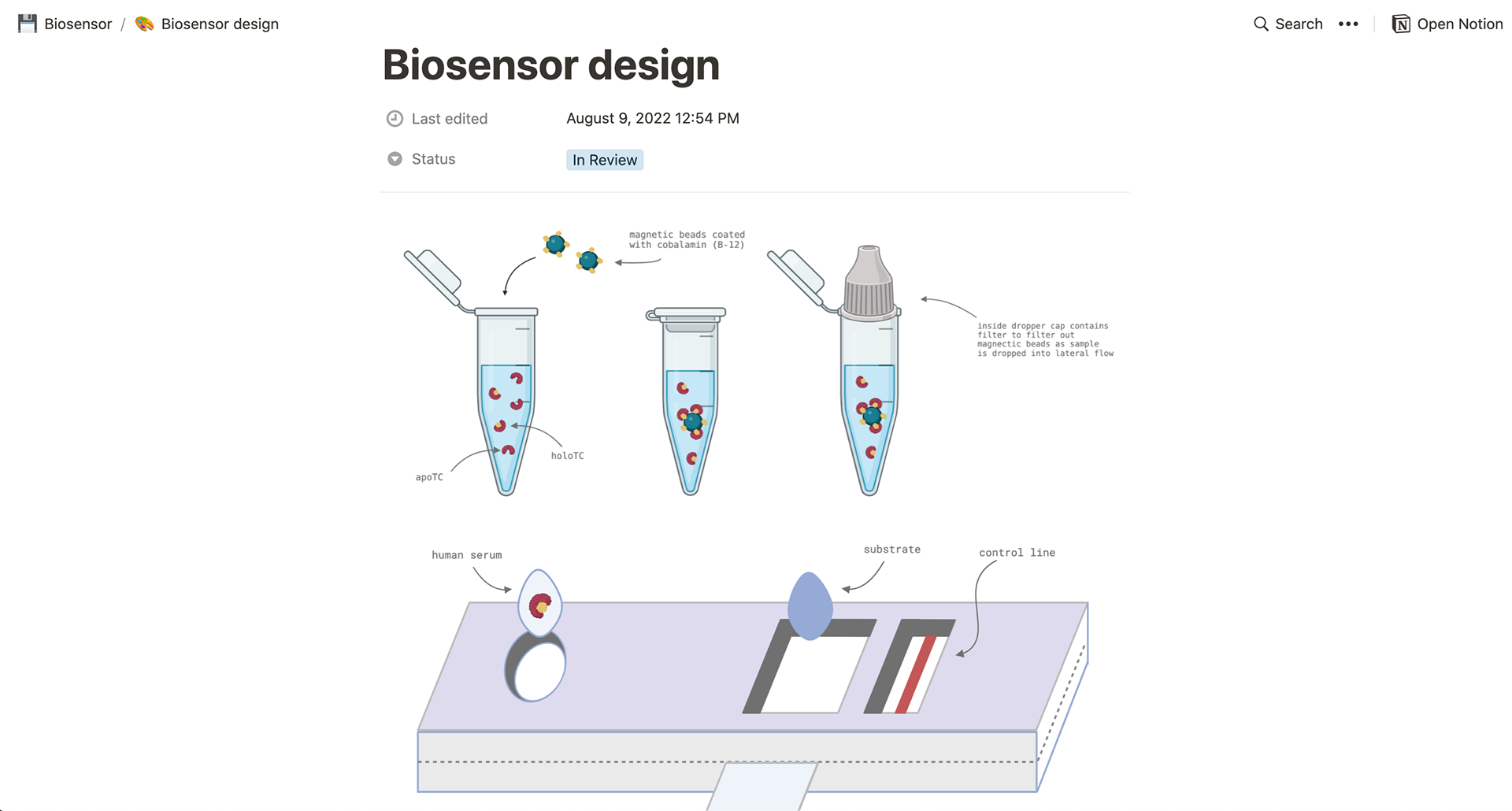
In enabling in-country assessment and reducing the cost per assay to <$5 USD with a low-cost biosensor, national surveys could reach $250,000, allowing actionable data to be collected every 2 years. This cost would be achieved via leveraging common resources like paper (remodeling the pregnancy test) and off-the-shelf glucometers.
First, we plan to target vitamin B-12, since it is the only micronutrient of public health concern (there are six) that does not yet have a low-cost assay developed specifically for low-resource settings that measures holoTC, its recommended biomarker. It also has the fewest number of programs established, both in Nigeria and across the majority of LMICs. So far the project has support from mentors at Harvard, MIT, The Knowledge Society, and cluB-12 UK, a group of B-12 scientists.